

John Meredith, Interoperability Specialist at EY, joined Part One of Understanding Patient Data’s EHDS Unpacked webinar series to bring the complex challenges of interoperability to life in a tangible way. Below he shares key themes spoken to in his presentation.
Interoperability across borders
Interoperability means making sure different health systems and IT systems can “talk to each other” and share information in a way that is useful. For example, it’s what allows your medical history to be understood and used if you receive care in another hospital – or even another country – without information being lost, misread or needing to be re-entered.
The European Health Data Space (EHDS) is an ambitious and necessary framework to align systems across 29 different countries (member states), and subsequently support interoperability. But making systems truly work together in practice doesn’t happen automatically just because a law exists or a technical standard has been agreed. From my experience in the NHS and across European programmes, real interoperability only works when three things are continuously aligned and maintained: policy goals, technical standards, and the ability to deliver them in practice.
For the UK, the key issue is how closely we stay aligned strategically. Developments in Europe will still influence the technology suppliers use, how systems are designed, and what the public comes to expect. The UK doesn’t need to formally be part of the EHDS for it to shape what we build – interoperability is already part of our day-to-day reality, not just a Europe-only policy discussion.
The pillars behind meaningful data exchange
Interoperability is often framed as a technical problem. In reality, it is a layered challenge. Semantic alignment (maintaining consistent meaning), clinical workflow integration, governance, accountability, and organisational capability matter just as much as application programming interfaces (APIs) and message formats.
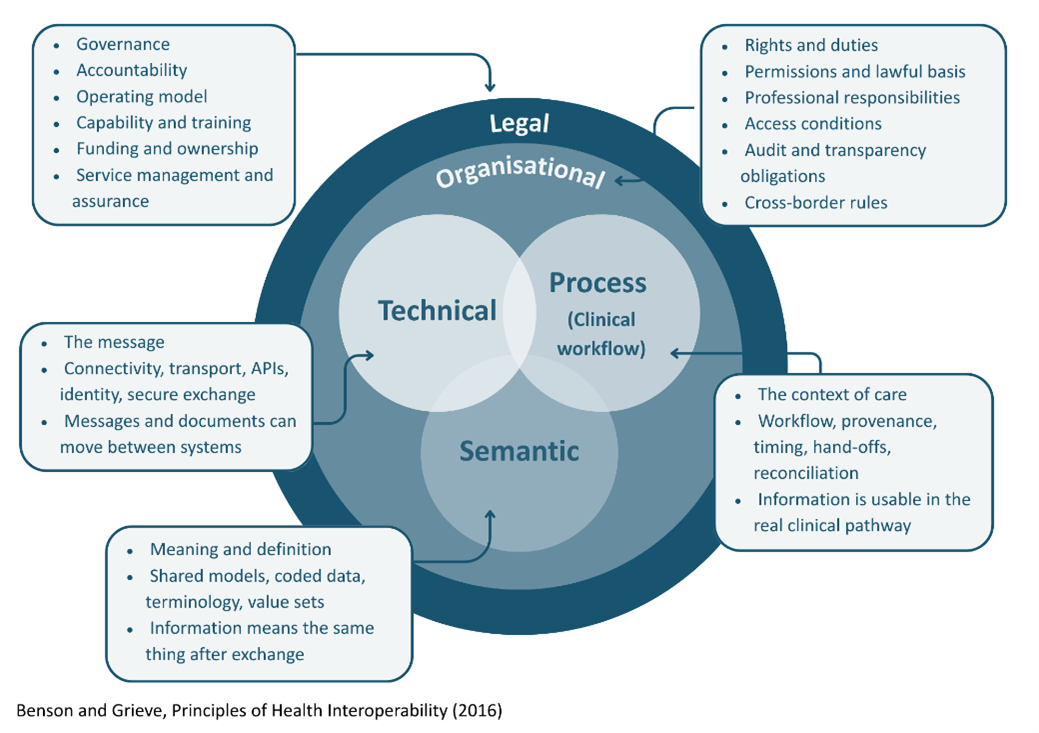
Standards like HL7 FHIR, SNOMED CT and openEHR each play important but distinct roles and none of them, on their own, guarantee safe and reliable exchange. The hardest work sits in areas that are often less visible but most critical: governance, conformance, operational ownership, and change management.
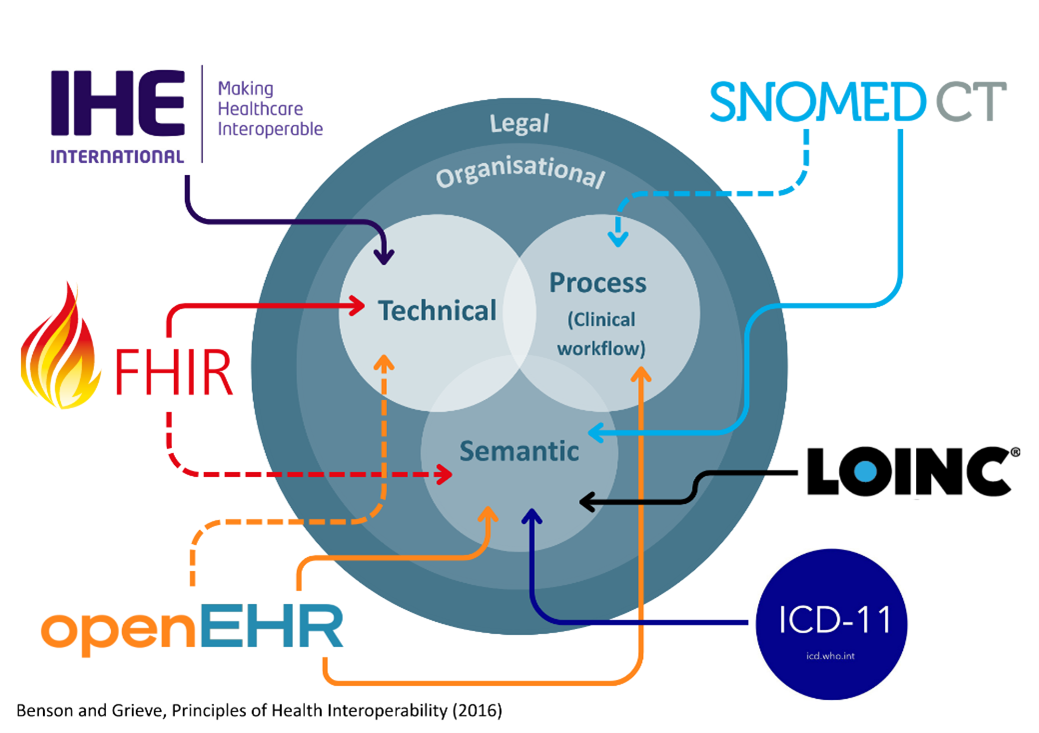
To be explicit about those distinct roles:
- HL7 FHIR supports structured exchange (e.g., APIs and information models for transfer and integration).
- SNOMED CT supports clinical meaning and semantic consistency across settings.
- openEHR supports persistent clinical modelling for structured, queryable records.
- LOINC supports consistent coding of tests, measurements and observations, especially lab results.
- ICD‑11 supports classification of diagnoses and related health problems for reporting and comparability.
- IHE supports implementable interoperability patterns (‘Integration Profiles’) that combine standards to support real workflows (e.g., XDS.b for cross‑enterprise document sharing).
In practice, interoperability depends on how these are combined within an architecture and not on selecting any one standard in isolation.
A key (often overlooked) point is conformance. Conformance is not just declaring alignment to a standard; it means validating structures, terminology bindings, and behaviour against agreed specifications, and doing so consistently. Without this, systems that are “FHIR compliant” on paper can still fail to interoperate safely in practice.
From datasets to dependable clinical exchange
Patient summary exchange is a good illustration of why this matters. On the surface, it sounds straight forward: retrieve and display a dataset. In practice, dependable exchange requires multiple foundations working together: verified identity, trusted access, agreed datasets, preserved provenance (tracking the data's origin and journey), shared terminologies, and safe presentation inside local clinical workflows. This is where policy, standards, and shared services intersect and where public trust is either earned or lost.
This leads to the concept of public digital infrastructure. When interoperability is approached as a set of shared, governed foundations (e.g., identity, registries, terminology services, validation, audit, and access control), rather than a series of one-off integrations, it enables scale and long-term sustainability. Crucially, interoperability becomes an enduring system capability, capable of being reused, governed, and continuously improved, rather than a one-time project activity.
The EHDS sets a clear direction and introduces obligations in specific areas, but member states still need to invest in national and regional capabilities to make exchange work for clinicians and citizens in day-to-day practice.
Time to align
While the EHDS is shaping important rights around transparency, control and patient governance, those rights only truly exist when they are delivered through usable, trusted services that people can experience in practice.
Encouragingly, many of these principles closely align with work already underway in the UK – from trusted research environments and open standards to patient‑centred governance and an increasing recognition that architecture matters. The task now is to be intentional in aligning efforts, learning from shared experience and actively engaging with the EHDS, so that we shape the direction of travel rather than simply respond to it.
Find out more about Understanding Patient Data's engagement with the European Health Data Space, and catch up on EHDS Unpacked Part One: What Europe’s health data future means for the UK.